Many Rx Opioids – Not Just Suboxone – Raise Risk of Dental Disease
/By Pat Anson
Suboxone isn’t the only opioid medication linked with dental decay and disease.
A large study led by VA Connecticut researchers found that patients on long-term opioid therapy with pain medications such as morphine and oxycodone have a significantly higher risk of infection-related dental disease.
The observational study included data from over 2 million U.S. veterans, 36% of whom were on long-term opioid therapy (LTOT). Those taking opioid pain medication for at least 90 days had a 24% higher chance of tooth decay, infections or tooth loss.
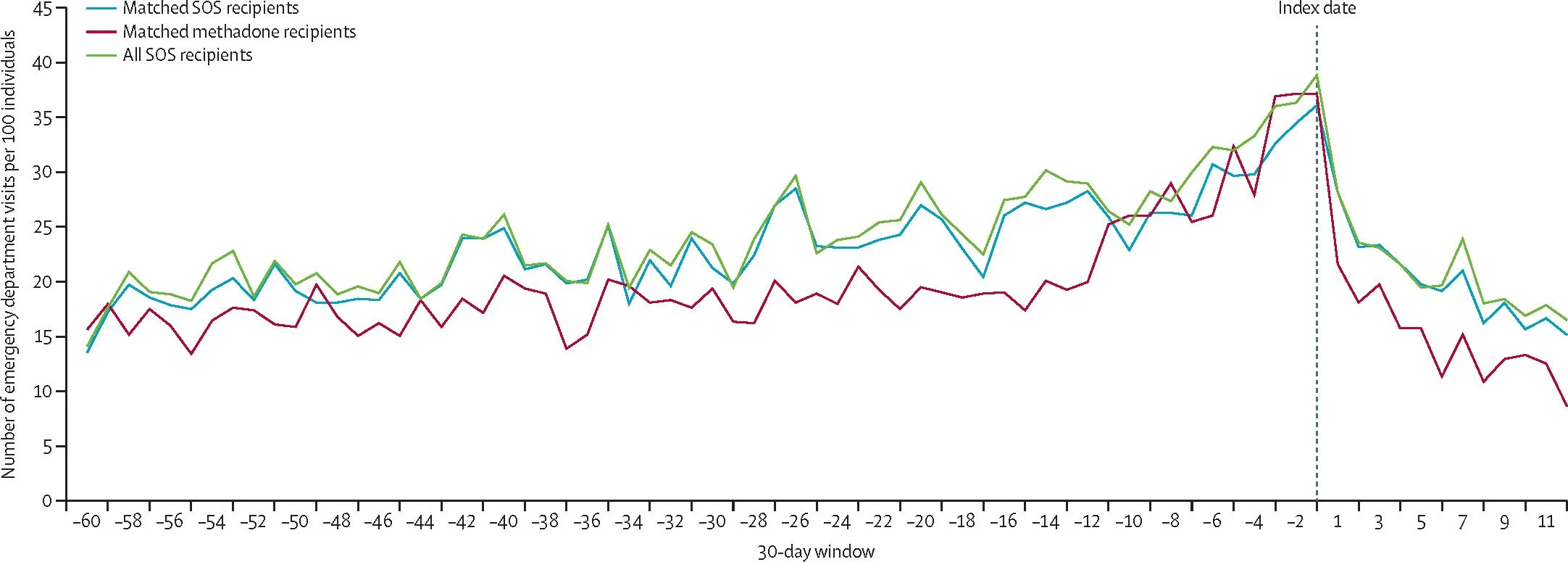
Suboxone, which contains the partial opioid agonist buprenorphine, was excluded from the study, along with the opioid methadone. Both medications are used to treat opioid use disorder (OUD).
The FDA warned in 2002 that buprenorphine tablets and film, when dissolved in the mouth, were linked to serious dental problems, including tooth decay, cavities, oral infections, and loss of teeth. Methadone has also been associated with dental problems because it induces dry mouth (xerostomia), which reduces saliva needed to wash away bacteria and plaque.
The new study is believed to be the first linking dental disease to opioids taken long-term for pain relief.
“To our knowledge, this is the first study to demonstrate the association between LTOT exposure and dental disease. This finding is important in light of recent warnings of buprenorphine risks that may influence decision-making in the context of chronic pain and/or OUD,” researchers reported in the journal PLOS One.
In their analysis, VA researchers compared veterans who took 12 opioids (hydrocodone, oxycodone, morphine, fentanyl, hydromorphone, dihydrocodeine, meperidine, pentazocine, propoxyphene, levorphanol, tramadol, or tapentadol) to veterans who had no exposure to LTOT in the prior year.
Researchers think the higher rate of dental disease for those on LTOT stems from immune suppression and reduced saliva flow, which raises the risk of bacterial infections that lead to dental disease and cavities.
The findings suggest that all patients on LTOT – whether for pain relief or OUD treatment – should be cautioned about the risks of dental problems.
“Concern over these risks may present a barrier to buprenorphine initiation in patients prescribed LTOT for whom such treatment is indicated. However, full opioid agonists themselves may pose oral health risks due to immunosuppression and well-documented effects on saliva flow causing xerostomia; both create opportunity for oral disease development,” researchers concluded.
Doctors who have patients on LTOT are advised to monitor their oral health and to have discussions with patients about dental risks before starting them on opioids.
There are simple steps patients on long-term opioids can take to reduce their risk of dental disease. Patients on buprenorphine or methadone are often advised to drink more water to combat dry mouth, and to brush and floss regularly to help prevent dental infections.