
As Pandemic Emergency Ends, People with Long Covid Feel Abandoned
/By Jackie Fortiér, KFF Health News
Lost careers. Broken marriages. Dismissed and disbelieved by family and friends.
These are some of the emotional and financial struggles long covid patients face years after their infection. Physically, they are debilitated and in pain: unable to walk up the stairs, focus on a project, or hold down a job. Facing the end of the federal public health emergency in May, many people experiencing lingering effects of the virus say they feel angry and abandoned by policymakers eager to move on.
“Patients are losing hope,” said Shelby Hedgecock, a self-described long covid survivor from Knoxville, Tennessee, who now advocates for patients like herself. “We feel swept under the rug.”
The Centers for Disease Control and Prevention estimated in March that 6% of U.S. adults, or about 16 million, were experiencing long covid, or ongoing health problems that continue or emerge after a bout of covid-19. Researchers estimate that 1.6% of U.S. adults, or about 4 million, have symptoms that have significantly reduced their ability to carry out day-to-day activities.
While patients are no longer contagious, their health issues can stretch on and affect almost every system in the body. More than 200 symptoms and conditions, including fatigue and depression, are linked to long covid, said Linda Geng, a physician who treats patients at Stanford Medicine’s Post-Acute COVID-19 Syndrome Clinic.
The severity and duration of long covid vary. Some people recover in a few weeks, while a smaller number have debilitating and lingering health issues. There is currently no test, treatment, or cure. There’s not even an accepted medical definition.
“When you don’t have any tests that show that anything’s abnormal, it can be quite invalidating and anxiety-provoking,” Geng said.
The physical and emotional toll has left some feeling hopeless. A 2022 study of adults in Japan and Sweden found that those with post-covid conditions were more than twice as likely to develop mental health issues, including depression, anxiety, and post-traumatic stress, as people without them.
“One of my friends committed suicide in May of 2021,” Hedgecock said. “She had a mild covid infection, and she progressively had medical complications continuously pop up, and it just got so bad that she decided to end her life.”
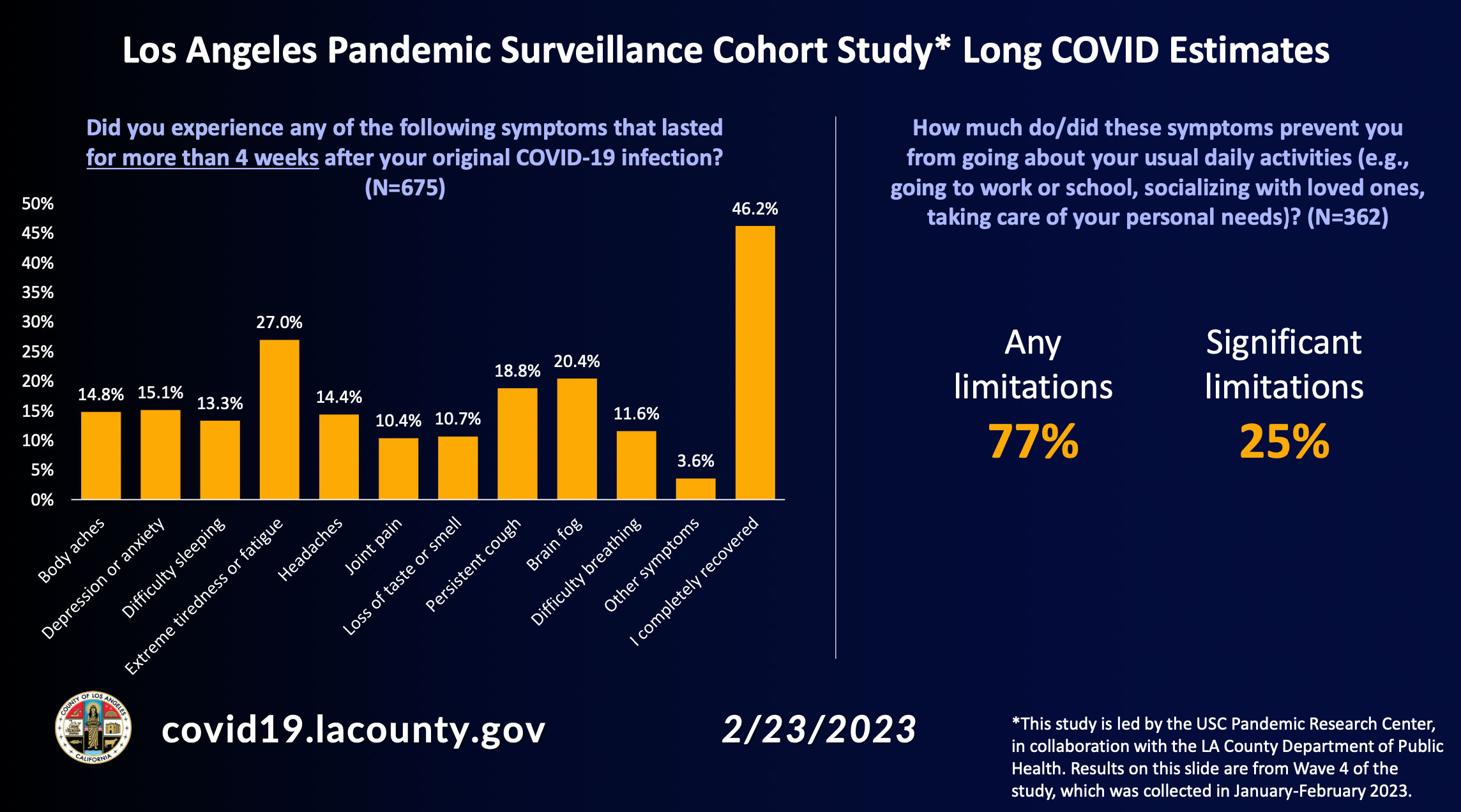
In Los Angeles County, 46% of adults who contracted covid were fully recovered a month later, but the rest — a majority — reported one or more continuing symptoms, according to a 675-patient study by the University of Southern California’s COVID-19 Pandemic Research Center. The researchers found chronic fatigue topped the list of health issues, followed by brain fog and persistent cough, all of which affect people’s daily lives.
Among the respondents who identified as living with long covid, 77% said their condition limited daily activities such as going to school or work or socializing. One-quarter reported experiencing severe limitations.
Taking antivirals cuts the risk of developing long covid in people who are newly infected. But for people already suffering, medical science is trying to catch up.
Here’s a look at Hedgecock and two other patients who have had long covid for years.
A Debilitating Brain Injury
Before contracting covid during spring 2020, Hedgecock’s life revolved around fitness. She worked as a personal trainer in Los Angeles and competed in endurance competitions on the weekends. At 29, she was about to launch an online wellness business, then she started having trouble breathing.
“One of the scariest things that happened to me was I couldn’t breathe at night,” Hedgecock said. “I did go to the emergency room on three different occasions, and each time I was told, ‘You’re up and you’re moving. You’re young; you’re healthy. It’s going to be fine.’”
Her primary care physician at the time told her she didn’t need supplemental oxygen even though her oxygen saturation dipped below normal at night, leaving her gasping for breath and crying in frustration.
Her condition kept her from one of her favorite hobbies, reading, for 19 months.
“I couldn’t look at a page and tell you what it said. It was like there was a disconnect between the words and my brain,” she said. “It was the strangest, most discouraging thing ever.”

SHELBY HEDGECOCK
Months later, under the direction of a specialist, Hedgecock underwent a test measuring electrical activity in the brain. It revealed her brain had been starved of oxygen for months, damaging the section controlling memory and language.
Since then, she has moved back to Tennessee to be close to family. She doesn’t leave her apartment without a medical alert button that can instantly call an ambulance. She works with a team of specialists, and she feels lucky; she knows people in online long covid groups who are losing health coverage as Medicaid pandemic protections expire, while others remain unable to work.
“A lot of them have lost their life savings. Some are experiencing homelessness,” she said.
In Bed for a Year
Julia Landis led a fulfilling life as a therapist before she contracted covid in spring 2020.
“I was really able to help people and it was great work and I loved my life, and I’ve lost it,” said the 56-year-old, who lives with her husband and dog in Ukiah, California.

JULIA LANDIS
In 2020, Landis was living in an apartment in Phoenix and received treatment via telehealth for her covid-related bronchitis. What started out as a mild case of covid spiraled into severe depression.
“I just stayed in bed for about a year,” she said.
Her depression has continued, along with debilitating pain and anxiety. To make up for her lost income, Landis’ husband works longer hours, which in turn exacerbates her loneliness.
“It would be nice to be living somewhere where there were people around seven days a week so I wouldn’t have to go through days of being just terrified to be alone all day,” Landis said. “If this were cancer, I’d be living with family. I’m sure of it.”
Landis refers to herself as a professional patient, filling her days with physical therapy and medical appointments. She’s gradually improving and can socialize on occasion, though it leaves her exhausted and can take days to recover.
“It’s terrifying because there’s just no way of knowing if this is going to be for the rest of my existence,” she said.
‘I Felt Betrayed’
Linda Rosenthal, a 65-year-old retired high school paraprofessional, has long covid symptoms, including inflammation in her chest that makes breathing difficult. She has found it hard to get medical care.
She called and set up a treatment plan with a local cardiologist near her home in Orange County, California, but received a letter five days later telling her he would no longer be able to provide her medical services.
The letter gave no reason for the cancellation.
“I was so surprised,” she said. “And then I felt betrayed because it is terrible to get a letter where a doctor, although within their rights, says that they don’t want you for a patient anymore, because it causes self-doubt.”

LINDA ROSENTHAL
Rosenthal found another cardiologist willing to do telehealth visits and who has staff wear masks in the office even though the state rule has expired. The practice, however, is more than an hour’s drive from where she lives.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at Kaiser Family Foundation.



{kind=link}