CDC Social Media Campaign Backfires
/By Pat Anson, Editor
A social media campaign by the Centers for Disease Control aimed at raising awareness about the "epidemic" of painkiller abuse had the unintended effect of launching another campaign about the "pandemic" of untreated chronic pain -- and how the agency was failing to address it.
Last month the CDC encouraged people to "help us tell stories of the many people whose lives have been affected by prescription painkiller addiction or the death of a loved one."
The agency, which estimates that over 16,000 Americans die annually from painkiller overdoses, asked for stories to be posted on Facebook, Instagram and Twitter with the hashtag #RxProblem.
“Prescription drug overdose devastates individuals, families and communities,” said Erin Connelly, associate director for Communication at the CDC. “We’d like to get everyone talking and thinking about the risks involved with opioid painkillers.”
While painkiller addiction and overdoses are undoubtedly a public health issue, the #RxProblem campaign rubbed some activists in the pain community the wrong way.
"There are really two problems with prescription drugs. One is the problem of abuse. But the other problem is patients who have pain and have a legitimate medical need for these drugs and can't access them," said Bob Twillman, PhD, Executive Director of the American Academy of Pain Management.
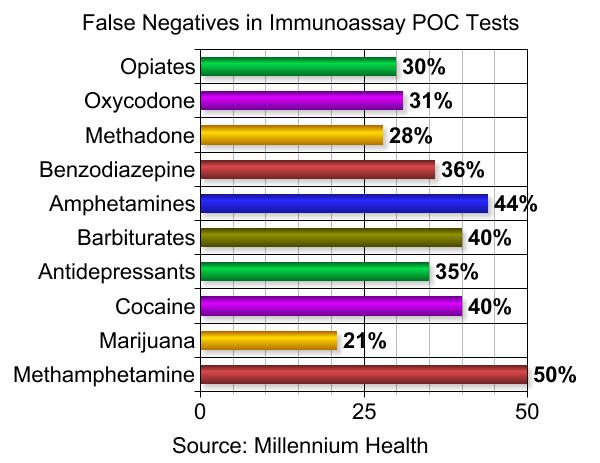
"I think they (the CDC) know what the problems are, but for some reason they don't want to deal with the chronic pain problem. I've criticized them for calling the problem of prescription drug overdoses and prescription drug abuse an 'epidemic' and taking a much, much bigger problem like chronic pain and not saying anything about it. Because to me, if 16,000 people a year dying from overdoses is an epidemic, then 100 million people with chronic pain must be a pandemic."
It was Twillman's idea to launch a rival social media campaign to draw more attention to the chronic pain problem.
"What we came up with was the idea of the hashtag #AnotherRxProblem, and have people who have trouble getting their medications write in about that experience and the impact that's had on them," Twillman told Pain News Network.
Write in they did, with hundreds of people complaining about the one-sided approach the CDC was taking to prescription pain medication.
"We need to live a quality life. Don't punish us. Find better pain control," posted Teri Daniel on Twitter.
"When will we take untreated pain seriously?" asked Melissa VanHouten.
"We have 2 public health crises: RxDrugAbuse & UnrelievedPain. Stop blaming. Work together," wrote Barby Ingle.
"We got a tremendous response. If you look at the Twitter feed for #RxProblem, about half of the posts are #AnotherRxProblem posts. We started another campaign on Facebook and the Facebook response absolutely blew up," said Twillman.
Dozens of pain patients also shared their stories on Dr. Jeffrey Fudin's blog.
"I’m going to get right to the point. PAIN AND OPIOIDS. They do help us. Yes, they’re in every group abusers and non-abusers. Those that it helps for medical necessity should not have to be punished, denied, etc. for those who choose to disregard the contract they signed," wrote Gina. "CDC there are alternatives, to wean out drug abusers. Utilize the resources you have vs. taking the easy way and punishing all."
The CDC's #RxProblem campaign officially ended May 15th. Did they get the message from #AnotherRxProblem get through?
"I'm not optimistic that it's going to make a change in what they're doing. But if it raises someone's awareness, then it was worth it," said Twillman.