Prescribed Opioids Not Linked to Veterans’ Heroin Use
/By Pat Anson, Editor
A new study of U.S. military veterans found a strong link between heroin use and the abuse of opioid pain medication, but with an important caveat: the heroin use was associated with the non-medical use of opioid painkillers.
Having chronic pain was also not found to be a significant risk factor for heroin use.
The ten-year study by researchers at Brown and Yale Universities followed nearly 3,400 veterans at nine Veterans Affairs facilities who were participating in the Veterans Aging Cohort Study (VACS).
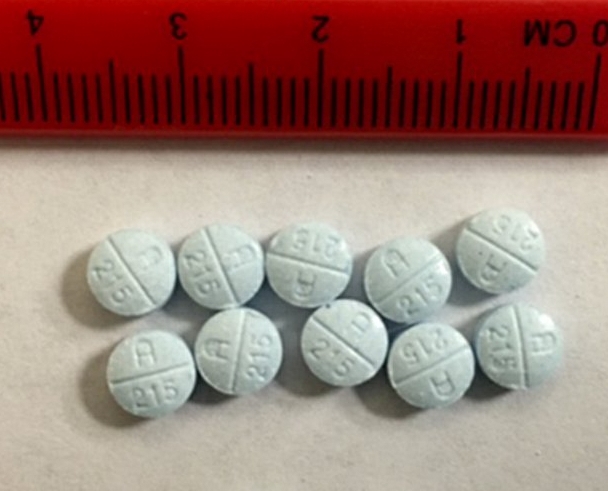
Of the 500 veterans who started using heroin during the study, 386 of them also began using prescription painkillers non-medically.
"Our findings demonstrate a pattern of transitioning from non-medical use of prescription opioids to heroin use that has only been demonstrated in select populations," said study co-author David Fiellin, a Yale public health and medical professor and director of the VACS study.
"Our findings are unique in that our sample of individuals consisted of patients who were receiving routine medical care for common medical conditions."

Even after statistically accounting for other risks -- such as race, income, use of other drugs, post-traumatic stress disorder (PTSD) and depression -- researchers found that veterans who began misusing painkillers were 5.4 times more likely to begin using heroin. Other major risk factors for heroin use include being male (2.6 times greater risk) and abusing stimulant drugs (2.1 times greater risk).
Veterans who received a short-term prescription for an opioid medication had a 1.7 times greater risk of starting heroin. But having a long-term prescription for opioids was not found to be a significant risk factor. And neither was having chronic pain.
“In our final model, pain interference in daily life was not a significant predictor of heroin initiation,” said lead author Brandon Marshall, an assistant professor in the Brown University School of Public Health.
Despite those findings, researchers recommend that all veterans should be screened for painkiller abuse, including those with legal prescriptions.
"This paper shows that, as a general clinical practice, particularly for this population which does experience a lot of chronic pain and other risks for substance use including PTSD, screening for non-medical painkiller use, whether you are prescribing an opioid or not, may be effective to prevent even more harmful transitions to heroin or other drugs," said Marshall, adding that veterans have a "constellation of risks" for substance abuse.
The study, published in the journal Addiction, did not identify the source of the opioids that were used non-medically. The National Institutes of Health and the U.S. Department of Veterans Affairs supported the study.
Under a federal spending bill passed by Congress and signed into law last year by President Obama, the Veteran’s Administration is required to follow the CDC's “voluntary” opioid guidelines, which discourage opioid prescribing for chronic pain. Since those guidelines were adopted, many veterans have complained to Pain News Network that their opioid doses have been reduced and they live in daily pain.
“They just cut my meds to one oxycodone every 12 hours, which gives me absolutely no relief,” wrote Harvey Williams, a Vietnam vet. “There must be something that the Veterans Administration can do to treat severe pain in the Vets. It's not fair for us to be sprayed with Agent Orange, return back to the United States, develop diabetes and in turn have severe neuropathy and pain for the rest of our lives and not be treated.”
“My VA doctors did not exam me prior to (cutting) my prescriptions,” wrote retired Army Capt. William Green, a Desert Storm veteran. “I asked how they decided to start reducing when I was reporting ongoing 6-8 on 10 pain scale. He didn't even consult with the doctor I do get ongoing treatment from. The doctor said, ‘We don’t care. We are following CDC guidelines.’”
The VA provides health services to 6 million veterans and their families. Over half of the veterans treated by the VA have chronic pain.