Pain Patient’s Death Was ‘State-Sanctioned Torture’
/By Richard “Red” Lawhern, Guest Columnist
Dawn Anderson was 53 years old and a former registered nurse. Her family has granted permission to share the story of her last days. Dawn’s story is both horrifying and highly representative of many people in pain. These are patients who – in effect, if not from deliberate intent – have died in entirely avoidable agony because of the CDC’s 2016 opioid prescribing guideline.
Dawn was diabetic. She also suffered from kidney disease. She had lost both legs and one eye, resulting in severe pain for many years, which until recently was managed with opioid pain relievers. Her pain management physician – Dr. Paul Madison -- is no longer practicing medicine. Madison was recently convicted of healthcare fraud and awaits sentencing for billing insurance companies $3.5 million for services he didn’t deliver. Madison reportedly had “pill mills” in 11 states, from which he dispensed very high volumes of opioids.
When Dr. Madison was barred from further treating patients, Dawn sought help from multiple pain management doctors in her area. She found that many were no longer accepting new patients. Among the few who would see her, none would treat her with opioids at the dose levels that had been effective for her in the past. Several were transitioning their patients to addiction treatment with Suboxone or recommending steroid shots.

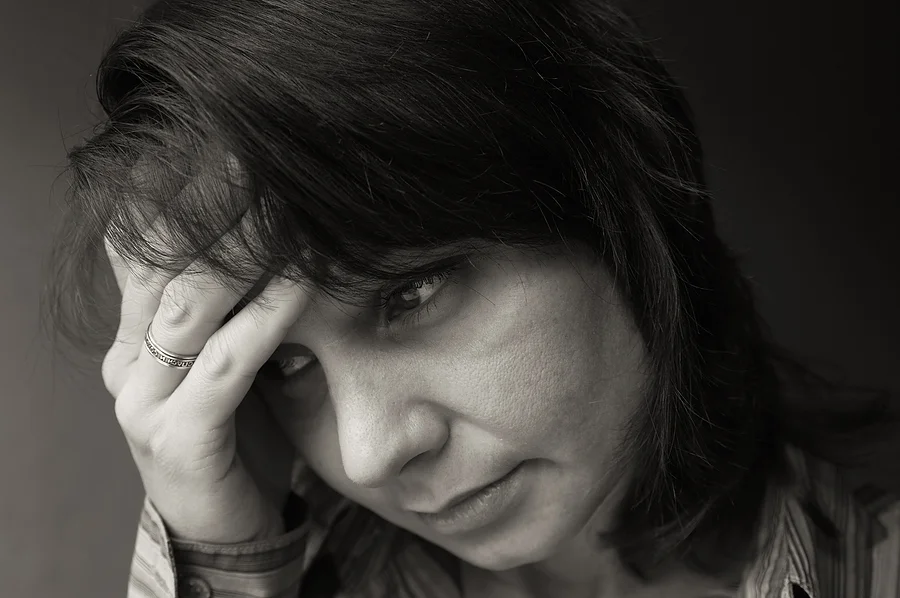
DAWN ANDERSON
Dawn’s most recent pain management doctor refused to prescribe above 90 morphine milligram equivalents (MME) per day, citing the CDC guideline as a de facto maximum allowable dose level.
Like many patients with chronic pain, Dawn’s medical situation was complex and involved several interacting medical disorders and issues. She had a history of MRSA – a highly aggressive antibiotic-resistant staph infection. Dawn had also personally observed many patients in whom spinal injections had led to worsening pain. She refused both Suboxone and the steroid shots
On March 4, 2019, a family friend spoke with Dawn. She was very tired and not feeling well. Her husband was calling from work throughout the day. When she did not answer, he called the police department and asked for a wellness check. When police arrived, they found Dawn had fallen out of her wheelchair and was unconscious on her living room floor. She was transported to a hospital. When she regained consciousness, she was very confused.
Hospital physicians determined Dawn had a severe urinary tract infection and her kidneys were failing. She was admitted to ICU and a doctor ordered a dialysis tube. Staff also forcibly started her on Thorazine injections, as she was refusing dialysis. They asserted that she was mentally incompetent. Family members observed that she was covered in bruises due to the force used when pinning her down to administer the injections.
On March 10th, Dawn was moved from intensive care to a regular hospital room. Her daughter called a family friend so that Dawn could talk to someone she liked and trusted. The conversation was very difficult. The friend asked why Dawn was refusing dialysis. Dawn replied, “I just can't take it anymore.” She anticipated having new issues with the dialysis, but most important was her unbearable pain. Hospital staff had again refused to provide adequate treatment with opioid pain relievers.
Both Dawn and her friend were in tears, but Dawn was adamant: “Honey, I love you, but I can’t suffer any more. The pain is unbearable and I just can’t fight any more. If you keep begging me to, I will hang up.”
Dawn’s friend and her family had talked with her about entering hospice care, where she would at least be treated for her pain. She was released from the hospital that day to go home. Her friend spoke with Dawn an hour later. She was tired, but had at last been placed on comfort care.
Dawn died a day later, on March 11, 2019.
What can we learn from this deeply disturbing narrative? Would Dawn have lived longer if she had been treated adequately with opioid pain relievers? That is impossible to say with confidence. But what is clear is that this woman died in needless agony. Dawn should never have been forced to see a pill mill doctor in the first place. And she should never have been forced to taper from effective dose levels because legitimate doctors were intimidated by CDC and state regulators into refusing effective — and largely safe — opioid therapy.
By any other name, this was state-sanctioned torture.
It is not accidental that the American Medical Association recently repudiated the CDC guideline. But the government dinosaur’s bureaucratic brain is in its tail and it hasn’t gotten the message yet. CDC has merely doubled down on the mythology that doctor over-prescribing caused our “opioid crisis.” They are running away from their own overdose data, which demonstrates the falsity of their assertion.
There is very little relationship between physician prescribing and either opioid addiction or overdose deaths. But the only metric CDC seems willing to use to measure the success of the war against drugs is reduced prescribing to Dawn Anderson and other people in pain.
It is time for this madness to stop! Opioid prescribing guidelines need to be taken away from the CDC and rewritten from the ground up by more competent agencies or by professional groups within medicine itself. And this time, multiple patient advocates need to be voting members of the writers’ group.

Richard “Red” Lawhern, PhD, has for over 20 years volunteered as a patient advocate in online pain communities and a subject matter expert on public policy for medical opioids. Red is co-founder and Director of Research for The Alliance for the Treatment of Intractable Pain.
The information in this column should not be considered as professional medical advice, diagnosis or treatment. It is for informational purposes only and represents the author’s opinions alone. It does not inherently express or reflect the views, opinions and/or positions of Pain News Network.