Steep Cuts in Opioid Prescribing ‘Raises More Questions’
/By Pat Anson, PNN Editor
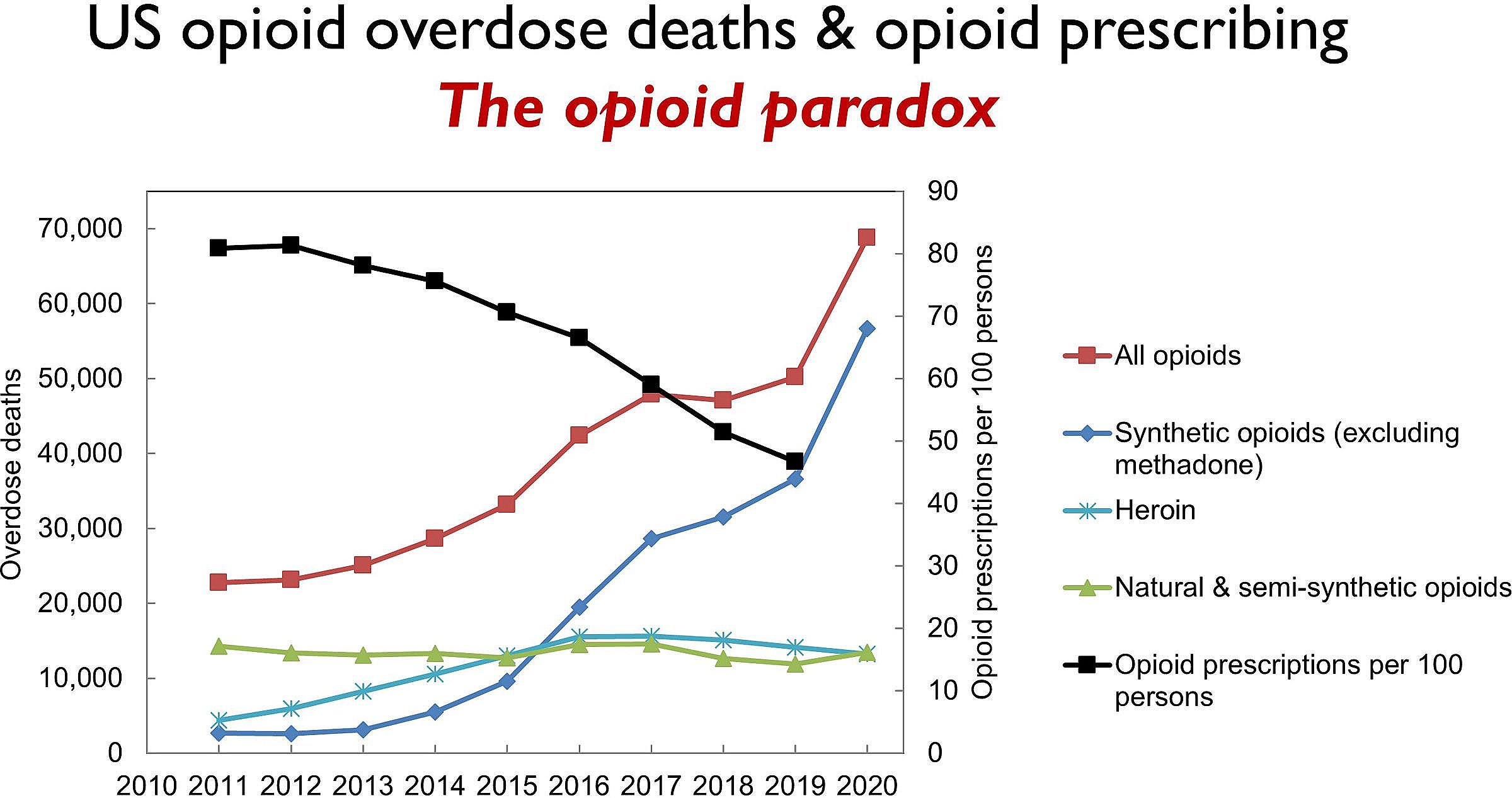
Several studies in recent years have documented how opioid prescribing has declined significantly in the United States, with per capita consumption of opioid medication recently falling to its lowest level in two decades.
For the first time, a new study by the RAND Corporation breaks the decline down by medical specialty, showing that some doctors may have gone too far in their effort to reduce opioid prescribing and lower the risk of abuse and addiction.
“Oftentimes when I do studies, I think we have a clear answer. This one in my mind raises more questions,” says Bradley Stein, MD, a senior physician researcher at RAND and lead author of the study published in the Annals of Internal Medicine.
Stein and his colleagues looked at opioid prescriptions filled at U.S. pharmacies in 2008-2009 and compared it to prescriptions filled in 2017-2018. Over that period, per capita morphine milligram equivalent (MME) doses for opioids fell by over 21% nationwide.
What surprised researchers is that many doctors treating patients with cancer pain, acute trauma pain or surgery pain significantly reduced their opioid prescribing even though most federal and state guidelines didn’t call for it.
The influential and much criticized 2016 CDC opioid guideline, for example, only applies to primary care physicians who treat chronic non-cancer pain. Yet emergency physicians, psychiatrists and oncologists cut their opioid prescribing significantly more than primary care providers and pain specialists.
MME Decline By Medical Specialty (2008 to 2018)
-70% Emergency Physicians
-67% Psychiatrists
-60% Oncologists
-49% Surgeons
-41% Dentists
-40% Primary Care Providers
-15% Pain Specialists
Stein attributes the steep decline in opioid prescribing not just to the CDC guideline, but to state regulations and insurance company policies. While some of the decline was appropriate, he thinks it may have gone too far.
“There are probably populations where a decade ago, someone may have given 30 days of opioids, where maybe 3 days or 7 days would be fine. Or maybe they didn’t need to prescribe it at all,” Stein told PNN. “But there are other populations for whom several days of opioids may very well be appropriate. And those are individuals that probably we should not be seeing substantial decreases in. An example is individuals with late-stage cancer.”
The CDC guideline specifically says it is “not intended for patients undergoing active cancer treatment, palliative care, or end-of-life care.” But in practice, many of those patients are being forced to follow the CDC’s recommended dose limits. Some get no opioids for pain relief. A recent study in Oregon found a significant decline in opioids being prescribed to terminally ill patients being admitted to hospice care.
“The blunt policy approach that called for reduced opioid prescribing across-the-board clearly affected some medical specialties more than others. But even patients receiving palliative care have felt the negative impact of opioid policies that have lacked nuance and depth,” says Dr. Chad Kollas, a palliative care specialist in Florida who has called federal opioid policy an “abject failure” because it has not reduced overdose deaths.
“Patients with cancer and sickle cell disease who are fortunate enough to have a palliative care physician still face challenges filling prescriptions for controlled pain medications at many pharmacies.”
PNN readers may be familiar with the story of April Doyle, a terminal breast cancer patient who posted a tearful video online after she was denied opioids at a Rite Aid pharmacy in 2019. Doyle went to another pharmacy and her prescription was filled, but only after a lot of unnecessary physical and emotional pain. She died the following year.
Geographic Variability
Another surprise uncovered by RAND, a nonprofit research organization, is the extreme variability of opioid prescribing from state to state and county to county.
The map below shows a checkerboard pattern across the United States, with counties in blue showing a 50% or more decline in opioid prescribing, and counties in red showing a 50% or more increase from 2008 to 2018.
Change in County Per Capita MME (2008-2018)

RAND CORPORATION
Per capita opioid prescriptions declined the most in large metropolitan counties (-22.6%) and in counties with higher rates of fatal opioid overdoses (-34.6%).
But even in states that were hit hard by the opioid crisis, such as West Virginia, Ohio and Kentucky, there are blue counties where prescribing fell significantly right next to red counties where opioid prescriptions spiked. Kansas and Missouri have more red counties than blue.
“It was eye-opening to see the variation across states and counties,” said Stein. “We’re seeing variation by payer. We’re seeing variation by community. We’re seeing variation by type of prescriber. And I think this is a reminder to us all that this is probably an issue where one-size-does-not-fit all.
“And I think coming to a better understanding of that will help us make sure that while we’re appropriately decreasing the amount of opiates being prescribed for people whose pain we can manage effectively in different ways, the decrease has been greater than it needs to be for some populations. We need to make sure that people who need adequate pain management get it.”
The RAND study was funded by grants from the National Institutes of Health.