Can Marijuana Improve Your Sex Life?
/By Roger Chriss, Columnist
A new study by researchers at Stanford University, published in the Journal of Sexual Medicine, shows that marijuana use is associated with greater sexual frequency in both men and women. There has been a lot of enthusiasm about the findings, but relatively little understanding of what the research actually says.
Marijuana has intriguing medical potential, from symptom relief in terminal cancer patients to pain management in chronic conditions. And the possibility that it may improve sexual function is enticing in particular for people with health problems. Thus, it’s important to understand what any new results are really saying. So let’s use this paper as a case study on how to read a research paper.
We start with the study methodology. Because the gold-standard of a double-blind placebo-controlled randomized prospective trial is not possible with marijuana, the authors had to engage in data mining, the process of using an existing data set to ask new questions.
For a data source, the study uses the National Survey of Family Growth (NSFG), a large database assembled by the CDC. The study results were drawn from an analysis of 28,176 women (average age = 29.9 years) and 22,943 men (average age = 29.5).
It is important not to be impressed by these large numbers. Increasing a sample size beyond a certain point offers no additional reliability, and it may create more problems with confounding variables and hidden biases. Because the authors did not assemble this data themselves, there was no way for them to address these issues.

A sanity check of the data is the next step. This study looks at sexual frequency at various levels of marijuana use. A check of the International Encyclopedia of Human Sexuality shows that “on average, men and women engage in sexual intercourse approximately six times per month.”
This is consistent with the Stanford study findings, but with a caveat: recall of the previous month’s sexual activity or marijuana use may be imperfect. Some researchers try to get around this problem by having participants keep written logs or by using apps, but this study did not.
It is also important to keep in mind that the study variable of sexual frequency is an imperfect number. You cannot have sex 0.73 times! Any change in sexual frequency has to occur in increments of one per unit time. In this study, the unit time is a 4-week period. The increase reported in the study represents the smallest possible increase, or one additional sexual event. The authors found that regular marijuana use was associated with one more sexual event every four weeks.
The study mentions the use of the NSFG data as a limitation. The authors note that “survey responses were self-reported and represent participants only at a specific point in time.” But there is a deeper issue here. As noted above, the data set may contain flaws, biases, or other issues beyond the control or even the awareness of the authors. Formally speaking, randomness is lost. In election polls, for instance, pollsters follow strict protocols to ensure randomness because doing so makes for more reliable results.
In practice, large data sets often contain many associations because life is complicated and even seemingly simple activities like sex are subject to a variety of influences. So posing questions to large data sets requires caution, or as statisticians sometimes say, “give me a large enough data set and I can prove anything.”
The Stanford study’s conclusion is that a “positive association between marijuana use and sexual frequency is seen in men and women across all demographic groups.”
But in an interview with The Washington Post, the authors qualify that by noting that the study “doesn't say if you smoke more marijuana, you'll have more sex,” appropriately warning that correlation is not causation.
Spurious Correlations
But the mantra of “correlation does not imply causation” is simplistic. In reality, association does not even imply direction. It is equally reasonable here to say that greater sexual frequency is associated with increased marijuana use. But changing the word order alters the implication.
The second problem is that the association may be meaningless, an artifact of our data-rich world. Such spurious correlations can even be a source of entertainment. For instance, coital frequency may be correlated with living in an even-numbered zip code or marijuana use may be associated with banana slug activity.
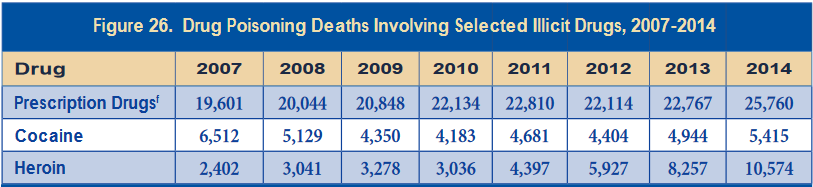
Not to make light of overdoses, but there is even a spurious correlation between deaths caused by opioids and the price of potato chips:

SOURCE: TYLERVIGEN.COM
These associations could be tested, but a positive result would probably not get the kind of media attention the Stanford study is receiving.
Moreover, sexual activity is influenced by a wide range of factors. It is possible that regular marijuana users have a lifestyle more conducive to sex, making lifestyle a lurking variable that affects both sexual frequency and marijuana use. Or it may be that daily marijuana users have more disposable income, more time to enjoy the effects of marijuana, and a more drug-tolerant work situation. In this case, marijuana use would act as a proxy for other potentially causal factors that influence coital frequency.
Because these issues are always found in large data sets, the potential for finding meaningless associations is ever-present. Or as statisticians say, “if you torture the data enough, you can get it to confess to anything.”
Thus, a study of this nature has inherent limitations that mean its results must be interpreted with caution. As the authors note in their conclusion, “the effects of marijuana use on sexual function warrant further study.”
So our final task is to consider what would constitute further study. Obviously, this result needs to be confirmed, ideally with a prospective study that controls for confounders. If the result is reproduced, then the hard work of identifying the causes begins. Once identified and confirmed through human testing, then and only then can we say that marijuana increases sexual frequency. For now the best we can do is read such studies with care and caution.

Roger Chriss lives with Ehlers Danlos syndrome and is a proud member of the Ehlers-Danlos Society.
Roger is a technical consultant in Washington state, where he specializes in mathematics and research.
The information in this column should not be considered as professional medical advice, diagnosis or treatment. It is for informational purposes only and represents the author’s opinions alone. It does not inherently express or reflect the views, opinions and/or positions of Pain News Network.